Monocyte
n., plural: monocytes
[ˈmɒnəʊˌsaɪt]
Definition: a phagocytic leukocytein the bloo, which may later develop into a macrophage or a dendritic cell
Table of Contents
Monocytes Definition
Monocytes are a subset of white blood cells (WBCs) or leukocytes that originate in the bone marrow. Monocytes are the largest type of white blood cells that act as a defender in the immune system by destructing or damaging the invading pathogen (viruses, bacteria, and fungi). Monocytes produce reactive oxygen species (ROS), nitric oxide (NO), myeloperoxidase, and inflammatory cytokines to kill pathogens.
Monocytes are considered cells of first-line defense against pathogens. Monocytes engulf the attaching pathogen due to its phagocytic nature. The plasma membrane of monocytes helps to engulf the pathogen followed by its digestion or breakdown. Thus, monocytes function to remove dead cells, pathogens, dead or damaged cells, and cancer cells. Under certain conditions like cancer cells and inflammatory diseases, monocytes are capable of either stimulating or inhibiting T-cells response. Also, monocytes have been found to play a role in neovascularization and tissue repair.
All vertebrates have monocytes. By population, monocytes are 5% of the nucleated cells present in adult blood. Thus, monocytes are an integral part of the innate immune system that also helps to maintain cellular homeostasis, especially during any inflammatory condition like an infection. The average half-life of monocytes is approximately 1 to 3 days.
Monocytes are WBCs that have innate plasticity to transform into macrophages or dendritic cells depending upon the milieu. Recent research suggests that monocytes can also differentiate into osteoclasts.
Monocytes are the largest cell subset present in the WBC with a typical size ranging from 13 to 25 μm in diameter. It may have an amoeboid appearance. Its nucleus is uni-lobulated. The chromatin has a lacy pattern. When stained with conventional dyes, the cytoplasm appears blue-gray in color with fine, red-blue azurophil granules. Vacuoles are usually present. Monocytes are produced in the bone marrow and function as a defender of infection and inflammation in the body. Monocytes eliminate the pathogens from the body by differentiating into macrophages while presenting the antigen to T lymphocytes by transforming into dendritic cells.
Overview:
Hematopoiesis is the process of forming new blood cellular elements in vertebrates. It begins with a multipotent stem cell, a hemocytoblast, which gives rise to a common myeloid progenitor cell (CMP). The CMP, in turn, gives rise to granulocyte-monocyte colony-forming units (CFU-GM), also called granulocyte-macrophage progenitor. The CFU-GM may partially differentiate into CFU-G (a precursor in myelocyte-granulocyte series) or CFU-M (a precursor in the monocyte-macrophage series). The CFU-GM serves as the precursor for monoblasts and myeloblasts. In the monocytic series, the monoblast is a precursor cell for promonocyte. The promonocyte matures into a monocyte. The monocyte migrates from the bone marrow to the peripheral blood through diapedesis. In humans, it constitutes 2% to 10% of the white blood cells in the body. In humans, some of the monocytes are stored in the spleen. As a type of white blood cell (leukocyte), the monocyte belongs to the mononuclear leukocytes as opposed to other white blood cells that are polymorphonuclear.
Structure
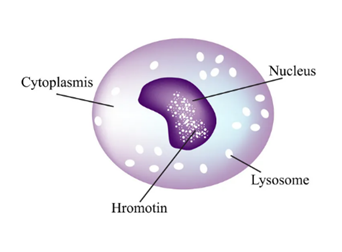
Monocytes are the largest of the white blood cell having a diameter of 12 to 20 µm (roughly estimated to be twice the size of red blood cells (RBCs)). Monocytes are mononuclear structures that have an ellipsoidal or kidney-shaped nucleus. Monocytes have a high nucleus-to-cytoplasm ratio (approximately 3:1). Monocytes are amoeboid structures having non-granulated cytoplasm and are hence sometimes referred to as agranulocytes. Although, sometimes, monocytes contain small azurophil granules scattered in the pale blue cytoplasm (Figure 1).
Development
Monocytes develop from the rapidly proliferating monoblasts in the bone marrow. Monoblasts are the precursor cells of monocytes that differentiated from hematopoietic stem cells. Once the development of monocytes is completed in 1-3 days they then briefly circulate in the blood for a duration of 1 to 1.5 days.
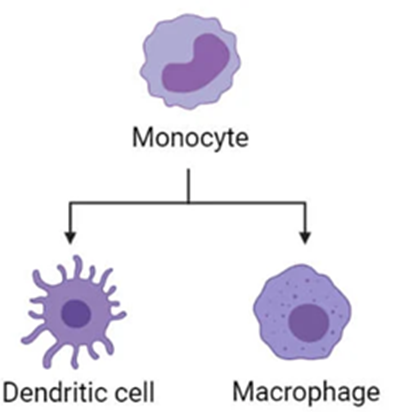
The expression of certain cell adhesion molecules and chemokines on the surface of monocytes leads to their exit from the bone marrow into general blood circulation. Subsequently, the monocytes then migrate to the specific tissue to differentiate into dendritic cells or macrophages (Figure 2).
Subpopulations
Let’s learn about the subsets or subpopulations of monocytes in humans and in mice.
-
In humans
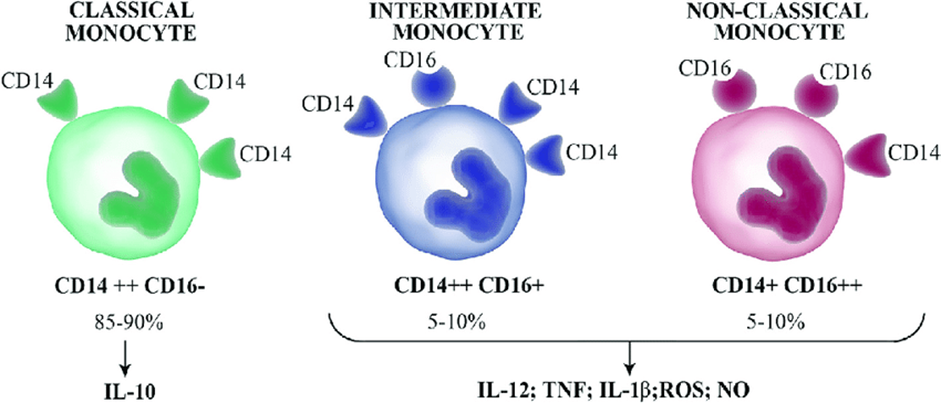
CD14, a glycoprotein, is the primary marker for human monocytes. CD14 is a myelomonocytic differentiation antigen that acts as the primary accessory protein for the toll-like receptors. Earlier it was thought that only CD14 is expressed in the monocytes, however, recent studies indicate that CD16 is also expressed in some of the monocytes. CD16 or the Fcγ receptor III, belongs to the Ig superfamily, which functions in antibody-dependent T-cell cytotoxicity (ADCC). The CD16 is involved in the antibody-mediated opsonization of uptake and clearance of pathogens. Thus, based on the differential expression of CD14 and CD16, human monocytes are now classified into three subtypes (Figure 3):
-
- Classical monocytes CD14++CD16− (also referred to as CD14+ or CD14+CD16−). Here, a high level of CD14 expression is seen. This represents almost 90% of the monocytes. Classical monocytes have been found to exhibit superior phagocytic and myeloperoxidase activities along with the high level of production of superoxides.
- Intermediate monocytes CD14++CD16+ (also referred to as CD14+CD16+ or CD14+CD16int/low). Here, CD14 and CD16 are co-expressed. This represents almost 10% of the monocytes population. Intermediate monocytes exhibit the highest level of expression of IL-12 and IFN-γ.
- Non-classical monocytes CD14+CD16++ (also referred to as CD14LowCD16+ or CD14dimCD16+) monocytes. Here, high level of expression of CD16 while diminished expression of CD14. Non-classical monocytes distinctly increase the production of TNFα.
Earlier monocytes were considered to be a homogenous population, however, later research findings indicate that monocytes undergo sequential differentiation. Post exit from the bone marrow, classical monocytes first differentiate into intermediate monocytes that eventually differentiate into non-classical monocytes.
Recent studies have shown that expression of slan (6-Sulfo LacNAc) cell surface marker is a more specific marker to differentiate between classical and intermediate monocytes.
-
In mice
In mice, only two subsets of monocytes are found, namely:
-
- Inflammatory monocytes, which are equivalent to classical monocytes CD14++CD16−. These are represented as CX3CR1low, CCR2pos, Ly6Chigh, PD-L1neg.
- Resident monocytes, which are equivalent to Intermediate or non-classical monocytes CD14++CD16+ or CD14+CD16+. These are represented as CX3CR1high, CCR2neg, Ly6Clow, and PD-L1pos. Resident monocytes are the patrolling cells found near the endothelial wall under a steady state as well as in an inflammatory condition.
Function
The primary functions of monocytes are as follows:
- Keep a watch for any microbes or pathogenic infection in the whole body i.e., patrolling. Monocytes slowly move along the endothelium to scan for the presence of any microbe in circulation.
- Stimulating other blood cells and immune response in case of infection and inflammation. This is usually done by dendritic cells that alert the other white blood cells and the immune system and make the whole body ready to fight the infection. Simultaneously, once a microbe was identified, macrophages are recruited to phagocytose the microbes/infected cells and also stimulate the production of cytokines.
Thus, monocytes serve the dual function of phagocytosis and antigen-presentation in the peripheral blood thereby ingesting and removing microbes, foreign material, and damaged or dead cells and killing cancer cells. Phagocytosis is the process of engulfing a solid substance in a cell and eventually digesting it.
-
Differentiation into other effector cells
As known, monocytes can differentiate either into macrophages or dendritic cells, depending upon the milieu. In case of infection, macrophages get differentiated into-
-
- Macrophages, for the purpose of eliminating the microbes by phagocytosis. Replenishing the resident macrophage population in the tissue is also one of the driving forces for the migration of monocytes in the tissues from the blood, especially during inflammation or infection. Macrophages are phagocytic cells having high anti-microbial activity. Macrophages are rich in the cytoplasm and contain a large number of vesicles to phagocytose foreign substances/microbes.
- Dendritic cells, in order to stimulate the immune system and prepare the body to fight against the infection by presenting antigens to the immune cells. Dendritic cells are antigen-presenting cells. The addition of cytokines interleukin 4 and granulocyte-macrophage colony-stimulating factor (GM-CSF) can transform monocytes into dendritic cells, in vitro. Also, it is important to note that monocyte-derived dendritic cells retain their transcriptome and form clusters with monocytes only.
-
Specific functions of monocyte subpopulations
All three monocyte subpopulations have different functions. In comparison to all the other subsets of monocytes, classical monocytes have the most phagocytic ability. Classical monocytes also produce high levels of myeloperoxidase and superoxides.
The intermediate monocytes are more involved in antigen presentation and stimulating T-lymphocytes. After phagocytosis, the microbial fragment combines with the Major Histocompatibility Complex (MHC) and is transferred to the surface of monocytes, which then present the microbial fragment /antigen to the T-lymphocyte to stimulate the immune response.
While the non-classical monocytes produce high levels of TNF-α.
Clinical Significance
Blood levels of monocytes estimated in a blood test is an indicative diagnostic parameter of blood disorders and other health conditions. The monocyte counts are often reflected in the complete blood count (CBC) test of the blood sample.
Monocytes in the blood can be expressed as a percentage of each cell in the blood or as an absolute monocyte count. Normal monocyte count is 1 to 10% of the blood cells.
Monocytes are estimated in a blood test known as white blood count differential. It has been reported that men have a higher number of monocytes as compared to women.
Nevertheless, the estimation of monocyte subset count is a more precise diagnostic tool for any disease condition like myocardial infarction (MI), multiple sclerosis, HIV, rheumatoid arthritis, tuberculosis, and other inflammatory conditions.
Monocytes is a vital part of innate immunity that plays both anti-inflammatory as well as inflammatory role. Hence, lack of, or abundance of monocytes is indicative of a pathological or inflammatory condition.
-
Monocytosis
An increase in the number of monocytes beyond the normal range or a high monocyte count is referred to as monocytosis. Microbial infection, i.e., fungal, bacterial, or viral infection results in monocytosis. Certain types of leukemia and its malignancy can result in monocytosis. Some of the disease conditions that exhibit monocytosis include viral fever, diabetes, chronic inflammation, stress response, atherosclerosis, Cushing’s syndrome (hyperadrenocorticism), sarcoidosis, immune-mediated disease, granulomatous disease, necrosis, red blood cell regeneration, chronic myelomonocytic leukemia (CMML).
In terms of a specific subset of monocytes, extremely high levels of non-classical monocytes i.e., CD14+CD16++ monocytes are indicative of sepsis or severe infection. High levels of intermediate monocytes, i.e., CD14++CD16+, are a cardiovascular risk indicator. In CMML monocyte count of > 1000/µL of blood is seen persistently.
Note it! Some drugs can increase monocyte count!
Certain drugs like corticosteroids, allopurinol, olanzapine, and Griseofulvin can cause monocytosis due to an increase in the levels of interleukins.
-
Monocytopenia
Reduction or deficiency in the number of monocytes is referred to as monocytopenia. Immuno-suppressive glucocorticoid therapy exhibit monocytopenia. Aplastic anemia use of myelotoxic drugs, acute infectious stress, myeloid leukemia, autoimmune diseases, and hairy cell leukemia also exhibit monocytopenia.
-
Blood content
Approximately 2 to 8% of the white blood cell count are monocytes which are almost equivalent to 200-800 monocytes/µL of blood (Figure 4).

Watch this vid about monocyte:
Take the Monocyte – Biology Quiz!

Further Reading
References
- Wacleche, V. S., Tremblay, C. L., Routy, J. P., & Ancuta, P. (2018). The Biology of Monocytes and Dendritic Cells: Contribution to HIV Pathogenesis. Viruses, 10(2), 65. https://doi.org/10.3390/v10020065
- Nahrendorf, M., Pittet, M. J., & Swirski, F. K. (2010). Monocytes: protagonists of infarct inflammation and repair after myocardial infarction. Circulation, 121(22), 2437–2445. https://doi.org/10.1161/CIRCULATIONAHA.109.916346
- Karlmark, K. R., Tacke, F., & Dunay, I. R. (2012). Monocytes in health and disease – Minireview. European journal of microbiology & immunology, 2(2), 97–102. https://doi.org/10.1556/EuJMI.2.2012.2.1
- Espinoza, V. E., & Emmady, P. D. (2022). Histology, Monocytes. In StatPearls. StatPearls Publishing.
©BiologyOnline.com. Content provided and moderated by Biology Online Editors.